Persistence pays off for HIV drug story


What sparked from a poster seen at a medical conference in 2023 eventually led to a news feature in 2025.
- Article: Will miracle HIV drug go on the PBS?
- Outlet: The Saturday Paper
- Length: 1400 words
- Turnaround time: Two days
- Number of interviews: Six
“When you’re saving a person’s life with a treatment, you can justify a very high cost on the basis of cost-effectiveness.”
Like many of my story ideas, this news piece was sparked by something I first saw at a medical conference. But it took two years, two rejections, and persistence before it finally got the attention I knew it warranted.
This piece highlights the importance of keeping tabs open – metaphorically-speaking – on stories that have the potential to develop further.
Why this story?
More than 40 million people worldwide are HIV-positive, and the virus still kills hundreds of thousands of people every year. Most of those with the disease, and those who die from it, are in low- and middle-income countries.
The moral tragedy/failure of HIV is that highly effective treatment and prevention options exist, but these are often unavailable, cost-prohibitive, or logistically challenging for the people who most need them. As a result, more than a million people – many of them newborn babies who acquire the disease in-utero or during breast-feeding – are infected with HIV each year. There are no effective vaccines against the disease.
That’s what makes this new drug, lenacapavir, so exciting. It’s a single, six-monthly injectable antiretroviral drug that is 100% effective at preventing infection and transmission. It’s not by definition a vaccine, but it’s the closest thing to it.
Lenacapavir is so effective at stopping HIV from replicating that the virus all but disappears from the body, so people with HIV don’t transmit the virus, and those without it who are taking the drug for prevention don’t get infected.
I was reporting on the 2023 International AIDS Society conference in Brisbane for Medscape, and hearing a lot of talk about long-acting injectables for both treatment and prevention, and how they had the potential to transform the HIV landscape. One poster ended up making the story list, because it looked at not only the huge potential benefits for HIV treatment and prevention, but about how to address the access issues relating to cost and availability.
Then at the 2024 Munich AIDS conference, some stunning data was released suggesting that a new long-acting six-monthly injectable – lenacapavir – was 100% effective at preventing HIV infection. I wasn't there, but I saw the coverage of it. This had the potential to be a true breakthrough for HIV treatment and prevention, but the going price was tens of thousands of dollars a year.
The pitch
Here’s the first pitch I sent to The Saturday Paper in July 2024:
There's some pretty important study results coming out of the AIDS 2024 conference in Munich this week, and one of those is the finding that a single injection of the antiviral lenacapivir is 100% effective at preventing HIV infection for six months in women and girls at high risk. It's the closest we've ever come to a preventive vaccine against HIV.
However, the going price for an annual course of lenacapivir in Australia and many countries is around $40,000-$50,000 year. Data presented at the conference suggests the mass production cost could be as low as $40.
The manufacturer Gilead has a direct voluntary licensing program that is supposed to enable easier access to the drug in some 'resource-limited' countries. But researchers at the AIDS2024 conference are showing that that program excludes many low and middle-income countries where the HIV epidemic is growing fastest. Around one-quarter of new HIV infections in 2022 were in countries not on Gilead's access list.
Gilead has form in charging exorbitant amounts for vital drugs: they were heavily criticised for charging $84,000 for a vital hepatitis C drug that cost less than $100 to manufacture.
In Australia, HIV infections have been steadily declining - there were 555 new infections in 2022 - which is good news. The uptake of PrEP among high-risk populations has had a major positive impact on infections, but that still requires a daily tablet so adherence is an issue. A six-monthly infection could transform HIV prevention, but not at that price tag.
Do you think there might be a story here for TSP?
That got crickets, but then I had another go in February 2025:
I pitched a version of this story to you last year, but it's now getting closer to reality so I thought I'd revisit it because there is a stronger news hook.
Lenacapavir is a six-monthly injectable antiretroviral drug that shows almost 100% effectiveness at preventing HIV infection in high-risk individuals. It's the closest thing to an HIV vaccine we've got and will likely have.
Last week, the manufacturer put an application into the US Food and Drug Administration to get the drug approved specifically for HIV prevention (it's currently only approved for treatment of drug-resistant HIV). If that goes through, Australia will likely follow suit. That could transform HIV prevention, and if it was made available to all high-risk individuals, we could see the end of HIV as a public health threat.
But there are some major barriers. The going price for an annual course of lenacapivir in Australia and many countries is around $40,000-$50,000 year. Data presented at the conference suggests the mass production cost could be as low as $40. For it to be accessible, it would have to be subsidised.
The rise in Christian nationalism around the world - especially in the US with Trump - makes that prospect uncertain. It also jeopardises the future accessibility of such a treatment in the parts of the world where it is most needed - low/middle-income nations where organisations like USAID were, until recently, the only supporter of HIV prevention and treatment.
What would a Lenacapavir mean in a nation like Australia, with relatively low rates of HIV – around 30,000 people living with HIV in 2023 – and high rates of testing and treatment? It's worth noting that HIV infections have been increasing since 2022, although are still low compared to other countries.
And what impact could the Trump administration's white Christian nationalism have on the fate of Lenacapavir globally, including in Australia?
Still no dice, but I kept the idea on the back-burner until June 2025, when:
So I think this is the third time I've raised this as a feature idea but there's a strong news hook now in that the US FDA yesterday just approved the antiviral lenacapavir as a six-monthly injection for the prevention of HIV.
This is the biggest game-changer in HIV prevention in a long time, because it's the closest thing to a vaccine that we've got. It's almost 100% effective at preventing infection, and has the potential to end transmission of HIV.
But there are some major barriers. The going price for an annual course of lenacapivir in Australia and many countries is around $40,000-$50,000 year, but the mass production cost could be as low as $40. This touches on arguments made about Covid vaccines, being that something that could save so many lives should not be a for-profit and that there needs to be a new IP model for access to such technologies.
With the FDA approving it, Australia's TGA likely won't be far behind. But as new HIV diagnoses continue to decline in Australia, what are the arguments for or against putting a drug like this on the PBS and making it accessible to all.
Let me know if you want more info, or if you think there's a story in this.
Finally, there was a strong enough news hook (or I simply wore the editor down), and I got the go-ahead for a 1400-word news story.
Where to start?
In some ways, this was a pretty straightforward story: new drug, amazing results, scientists happy, patients excited. It’s surprisingly rare how often that type of story is genuinely worth telling (as opposed to being a slick packaged story pushed by a drug company’s PR unit to generate sales).
But what made this more interesting was the equity aspects of the story. Lenacapavir’s price tag puts it out of reach of all but the most wealthy, echoing a pattern that has been seen since the earliest days of HIV treatments.
So while I started with the science, I knew that a big part of the story would be exploring the socioeconomics of the topic.
Interviews
Australia has some – many – stellar researchers and clinicians working in HIV prevention and treatment. I suspect that’s a legacy of Australia’s ground-breaking approach to tackling HIV when it first emerged, which directly involved the communities most affected by HIV in developing strategies to combat it, instead of being held back by stigma, ignorance, homophobia and fear.
That approach has continued to underpin how Australia has worked with pre-exposure prophylaxis, and more recently with m-pox. We are far from perfect, but we've got a lot of things right.
So I was spoiled for choice in finding researchers and clinicians to interview. But I wanted to cover some important angles, such as what the new drug meant for people with HIV and the communities and individuals at higher risk of infection. what it meant for people at risk in low- and middle-income nations, and whether the drug should or would be subsidised on the Pharmaceutical Benefits Scheme.
That meant also talking to representatives of those communities, and those who could comment on the socioeconomic and practical aspects.
Research
The research for this was pretty straightforward as well. I read the research papers and conference abstracts for the clinical trial data on lenacapavir and similar drugs, got my head around how they worked, and looked into what had been released and written about the cost. I also looked at the approval information from the US FDA and Australian TGA, and researched the stats on HIV infections in Australia and globally.
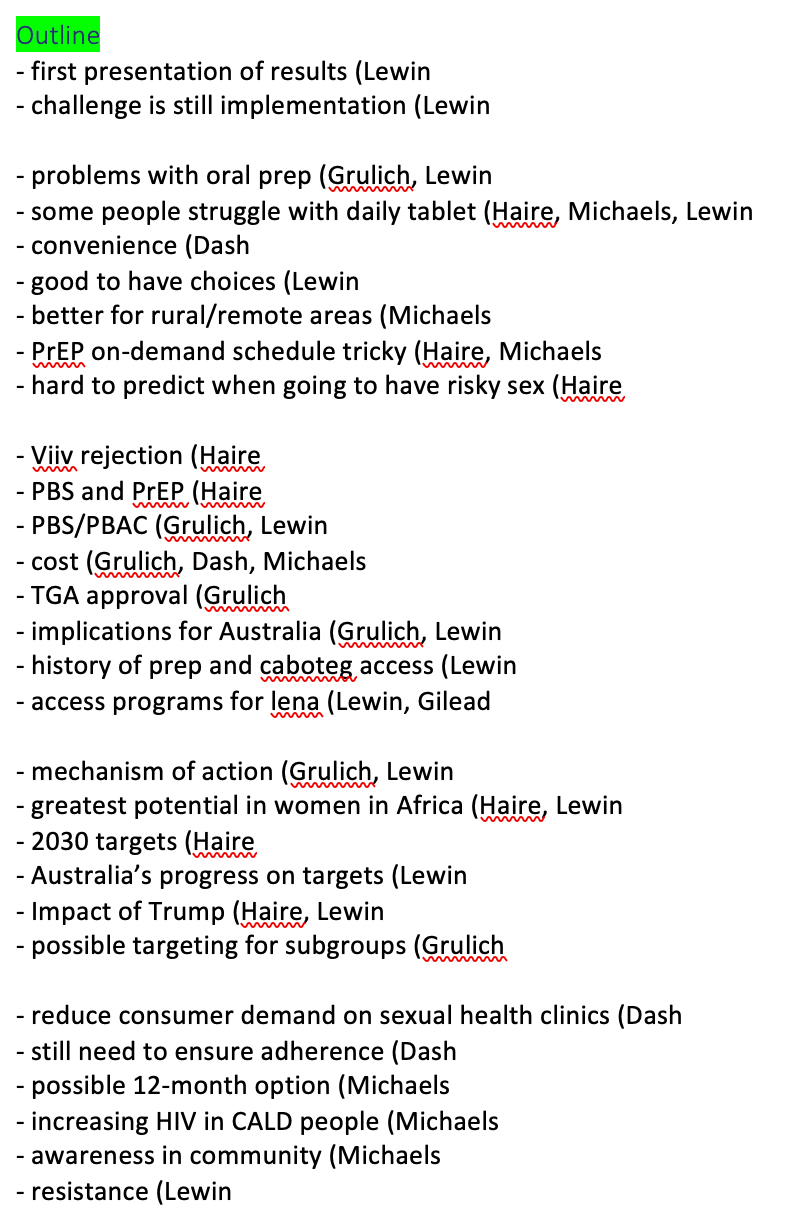
Structure and writing
Here’s the outline. Not everything made it into the piece, but that’s the tyranny of a tight word-count.
What did I learn from doing this?
Don’t give up on a good story. Sometimes it just takes time for the right news hook to come along, so keep your eye on things until it does.
And yes, I'm still keeping an eye out for whether this drug gets PBS listed for prevention. Watch this space.